
 FOCUS Speaks with Nathan S. Bryan, PhD, On Common Aetiologies of Inadequate Nitric Oxide Production, and the Problems It Causes
FOCUS Speaks with Nathan S. Bryan, PhD, On Common Aetiologies of Inadequate Nitric Oxide Production, and the Problems It Causes
Nathan S. Bryan, PhD, is an international leader in molecular medicine and nitric oxide biochemistry. Specifically, Dr. Bryan was the first to describe nitrite and nitrate as indispensable nutrients required for optimal cardiovascular health. He was the first to demonstrate and discover an endocrine function of nitric oxide via the formation of S-nitrosoglutathione and inorganic nitrite.
Dr. Bryan has been involved in nitric oxide research for the past 18 years, and he has made many seminal discoveries in the field. Many of these discoveries and findings have transformed the development of new therapeutic agents for the treatment and prevention of human disease.
Dr. Bryan has published a number of highly cited papers and authored or edited five books. More about his work can be found at www.drnathansbryan.com.
FOCUS: Let’s start with some basics here. Nitrites, nitrates, nitric oxide—what’s what, and how do they relate? Are these molecules good, bad, or potentially both?
BRYAN: There’s been an evolution of the perspective of nitrites and nitrates. Back in the 50s and 60s, we were taught these were dangerous food additives that formed nitrosamines, which caused cancer. Then, fast-forward to 30 or 40 years later, the National Toxicology Program put nitrites and nitrates through long-term safety trials and found no evidence of carcinogenicity whatsoever. Then, in the late 80s and early 90s, nitric oxide (NO) was discovered, and it was realised that nitrite and nitrate could be formed endogenously from NO.[1] This told us in the scientific community that nitrite and nitrate are part of the normal NO metabolism. NO really is one of the most important molecules produced in the human body—so important, in fact, that in 1998, the Nobel Prize in Physiology or Medicine was awarded for the discovery of NO. These things in the scientific community told us a lot about nitrite and nitrate: they weren’t toxic food additives that caused cancer, and they were actually really important metabolites that can be utilised (as we understand now) to form NO.
However, this message hasn’t necessarily translated to consumer awareness and the messaging of food companies or other forms of marketing. People thought for years that nitrites/nitrates were mainly found in cured and processed meats—but really the greater burden of exposure is from eating green leafy vegetables, and less than 5% of nitrites/nitrates that we are taking in is from bacon, hot dogs, or other cured and processed meats. In fact, this is the reason that a diet rich in vegetables can lower blood pressure, because these nitrites/nitrates are metabolised and converted to NO, and NO dilates blood vessels and lowers blood pressure.
If nitrites/nitrates were harmful, then we would see vegetarians having a higher incidence of cancer and cardiovascular disease. Epidemiological data shows this is not the case, and that vegetarians have lower rates of these conditions—which we now understand, mechanistically, may be due to the presence of nitrites/nitrates that increase NO levels in the body, improving vasodilation, blood flow, and even mitochondrial function.
So, the answer is that NO is good for you, as are nitrites and nitrates. These are all-natural molecules produced in the body.[2],[3] The data show us they actually have the opposite effects of what we were told 40 years ago: more than 160,000 published scientific papers show us that if your body can’t make NO, or if you are not getting enough nitrite/nitrate in your diet, this puts you at risk of every single age-related and chronic degenerative disease.
FOCUS: If nitrates are inert, and nitrites are what nitrates must convert to, why aren’t we advocating that people eat more bacon?
BRYAN: The problem is that you really can’t eat enough bacon to get the amount of nitrite/nitrate that the body needs to produce NO. NO has a half-life of about one millisecond,[4] so we need to constantly be making it. When we consider cured and processed meats, the potential culprit has always been nitrosamine, not nitrites and nitrates. However, nitrites can form nitrosamines under certain conditions. In modern meat-curing processes, when manufacturers add sodium nitrite to these products, they also add ascorbic acid or a structural analog known as erythorbate, compounds that prevent nitrosamine formation.[5]
If you are a meat eater and eat one to two servings of cured or processed meat weekly, the relative risk of cardiovascular disease, cancer, and all-cause mortality is about 1.15 to 1.23, although some studies show it may be even lower.[6],[7],[8],[9] At 1.15, this is probably within the noise, due to some confounder that probably wasn’t noted, and a moderate level of consumption of these things cannot be pointed to as causative.[10] For comparison, the relative risk of cancer associated with smoking or asbestos exposure is around 10 to 40.[11],[12],[13]
We see ads for things like nitrite-free bacon or organically cured sausages—but this is deceptive marketing because we need nitrites to preserve meat, and there are no replacements for nitrites. Despite using alternate processes to produce nitrites, these products still contain them.[14] Nitrites in these products prevent botulism, bacterial overgrowth, and lipid oxidation, and give these products a shelf life so we can eat them safely.5 Over the years, rather than adding sodium nitrite, manufacturers have added celery salt (which contains nitrate) and a starter culture of bacteria that converts nitrates to nitrites.[15] The challenge with that approach is that the level of protective nitrites is highly variable—the nitrate content of celery salt is variable; the bacteria activity is variable—giving them an unknown safety profile. It really is better to just use the original process because we have known for years that there is no evidence of toxicity from having nitrites or nitrates in the diet.[16]
All that said, when one eats a plant-based diet, they are not only are getting higher levels of nitrites and nitrates, they also are getting additional essential vitamins and minerals, and an abundance of polyphenols and phytonutrients that are found at higher levels in these foods and have important health effects. Additionally, the antioxidants found in plant sources of nitrates and nitrites not only naturally inhibit nitrosamine formation like ascorbate and erythorbate do,
FOCUS: In addition to diet, what are some of the main things that affect the body’s ability to produce NO?
BRYAN: The microbiome is really becoming more important to human health than we ever realised. People have been focusing extensively on the gut bacteria and how this impacts health for numerous years, seeing enormous benefits from things like faecal transplant and the use of probiotics to affect the gut microbiome. In our research, we focused on the oral bacteria because it is well established to play a role in NO production.
One of the things we discovered over the past decade is that people need the right type of oral bacteria to reduce nitrate (NO3-) to nitrite (NO2-), from which NO is produced (see Figure 1). The problem is that over 200 million Americans are waking up every day and using an antiseptic mouthwash to kill the bacteria in their mouth, which they have been told to do for good oral hygiene. However, when they do this, they are unknowingly killing the good, nitrate-reducing bacteria as well.[18],[19] They can do all the right things—exercise, eat lots of leafy vegetables—but, by using mouthwash regularly, they are effectively killing their body’s ability to make NO. Their blood pressure goes up, putting them at increased risk for heart attack, stroke, dementia, and all of the conditions that accompany poor blood flow.
We’ve really only studied chlorhexidine, the strongest antiseptic mouthwash on the market, which is available as a prescription for chronic halitosis.[20] We used this because we wanted to eradicate all the bacteria and see what happened. Other people have looked at things like alcohol-based mouthwash and found similar effects,[21] but we really don’t know about natural mouthwashes. It has been challenging to get funding for many of these studies. That said, there really is no mouthwash that I am aware of that selectively kills the bad guys and preserves the good guys that are needed to make NO.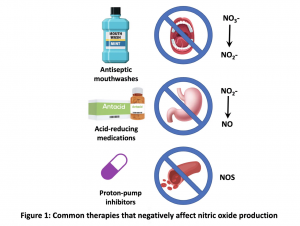
Another thing is that antibiotics do the same thing; if you take an oral antibiotic, you are not only killing the bad bacteria, but also the good. Antibacterial soaps and hand sanitizers — these things are also killing bacteria in your body that are doing very important things, such as producing NO.
Unfortunately, we have not been able to develop a probiotic that contains any of the bacteria we have determined to be important for the oral production of nitrites from nitrates. I have tested a lot of the probiotics that are on the market, and none contain these bacteria, either. We also haven’t found any probiotic strain that helps reestablish this good flora in the oral cavity, replenishing the nitrate-reducing bacteria.
Another major hurdle in NO production is the use of antacids and proton-pump inhibitors (PPIs). These drugs completely shut down NO production. Studies have shown that people who have been on PPIs for three to five years have a 35 to 40% higher incidence of heart attack and stroke.[22] This really creates a problem for clinicians because these drugs aren’t meant for chronic use, yet you can get many of them over the counter, and people use them daily because their reflux is intolerable. It’s really difficult to get people off these medications.
FOCUS: How do PPIs shut down NO production?
BRYAN: There are actually two ways they do this. When we swallow our saliva, it is enriched in nitrite, produced by the oral nitrate-reducing bacteria. When the saliva reaches the acidic environment of the stomach, nitrite becomes protonated and generates NO gas (see Figure 1).[23] But if the stomach is not acidic, then you are not generating NO in the lumen of the stomach.
The second thing PPIs do is inhibit an enzyme called dimethylarginine dimethyl-aminohydrolase (DDAH). This leads to an accumulation of asymmetric dimethylarginine (ADMA), which is a competitive inhibitor with arginine for the binding to nitric oxide synthase (NOS)[24]—so you’re also basically shutting down this pathway for production of NO, as well. So, PPIs do what no other drug has been shown to do and shut down total body NO production, which is a very bad scenario.
People have to get off these drugs because the body can’t heal without stomach acid. Additionally, if you take these drugs, you have poor absorption of vitamins and minerals in your foods; you can’t break down proteins to amino acids, so you get these peptide antigens absorbed across the gut, which is the basis for food allergies; you get Helicobacter pylori overgrowth and ulcerations; and some people can actually have reflux due to stomach acid suppression. In my opinion, these drugs are some of the most dangerous on the market today because they lead to the progression of so many chronic diseases. You really have to restore normal stomach acid production, or your body cannot heal.
FOCUS: What might be the first sign/symptom of someone having inadequate NO production?
BRYAN: The result of a decrease in NO production is a decrease in blood flow, and, clinically, this manifests in sexual dysfunction: erectile dysfunction in men and vasculogenic female sexual dysfunction in women.[25],[26] NO signals to blood vessels to open up and regulates blood flow upon demand. For regular sexual function, you need an increase in blood flow, which means you need to produce NO. If the endothelial cells and the nerve endings that innervate those organs can’t make NO, you can’t dilate the blood vessels and you can’t get an increase in blood flow. A high percentage of men over the age of 40 self-report erectile dysfunction, and there probably is another substantial percentage that don’t report because of the stigma they associate with it. Although it is often due to a more dynamic array of contributing factors, more than 40% of women aged 18 years or older in the U.S. also experience sexual dysfunction.[27]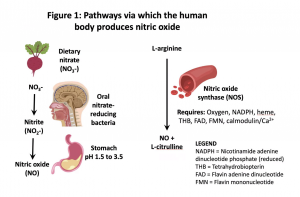
Because NO is a vasodilator and regulator of normal blood pressure, with inadequate NO production, blood pressure will increase. About 50% Americans have or are being treated for high blood pressure,[28] so this really is a lot of the population. Usually sexual dysfunction occurs before the increase in blood pressure.[29] As things progress, you begin to see this chronic inflammatory vascular disease with plaque deposition in the lining of the blood vessels, and the arteries become dysfunctional.[30] If you don’t correct this, the plaque becomes unstable, and can lead to a heart attack or a stroke, the number-one killer of men and women worldwide. So, there is a very clear progression of cardiovascular disease that begins with the loss of NO production and the loss of blood flow regulation. However, very few people know about NO and how to restore normal production, so it’s no wonder that cardiovascular disease is the number-one killer worldwide.
FOCUS: Is there a way of testing NO levels?
BRYAN: That’s part of the problem—you can’t go to your doctor and ask what your NO levels are; there is no standard lab test.[31],[32] What we have to do is rely on symptoms, so my mission has been to teach clinicians the signs and symptoms of NO deficiency. Now, there actually are FDA-cleared medical devices that can measure endothelial function,[33],[34] so this can give you a sense of what your NO production capability is. This is very important because once you diagnose NO insufficiency, you can address it before problems hit, because the loss of normal NO production precedes the structural changes by many years, sometimes even decades. So if you can assess whether patients are starting to show endothelial dysfunction in their 20s, 30s, and 40s, and you employ these lifestyle and therapeutic strategies to restore NO production and improve endothelial function, by all bets you can prevent age-related disease, particularly cardiovascular disease.
We developed NO testing strips a number of years ago, but the challenge was that no one knew what NO was. So, the patient or consumer would say “How do I know I need this?” The test was a simple saliva test strip: you apply your saliva to the end of it and if you have sufficient total body NO production it turns pink, if you don’t, it stays white and tells us you are NO deficient.[35]
It is a good biochemical test and something to have in your toolbox, but a functional test always outweighs a biochemical test. It tells us you are NO deficient, but doesn’t tell us is why: is it because you have endothelial dysfunction, does the enzyme in your blood vessels not work to make NO, are you not eating enough green leafy vegetables or nitrate in your diet, is it because you are using antiseptic mouthwash and killing the good bacteria? But what’s clear is that if you are depleted, you are depleted. So, then we eliminate the things that are inhibiting NO production and start doing things that promote NO: changing the diet, fixing stomach acid levels, getting moderate physical exercise, and potentially taking nutritional supplements that increase NO production.
FOCUS: Why is support for NO production important in the setting of age-related disease?
BRYAN: Mechanistically, every age-related disease, every single human chronic disease, has a vascular component.[36] Whether it manifests in the kidney, the brain, the heart, or the liver, there is one thing they all have in common: hypoxia or ischemia, or low blood flow. So, it’s a vascular problem.
Even Alzheimer’s and vascular dementia have this component – reduced blood flow to the prefrontal cortex. Over time, if you don’t fix and get blood flow to fire those synapses, you get dysfunction and lose your ability to recall memory. The common denominator in any brain/neurological disorder is a loss of regulation of blood flow, and that is all dependent on NO.[37],[38] In vascular dementia patients, we have shown hypoperfusion in certain regions of the brain with functional MRI, and employed NO-based technologies, and 30 days later the functional MRI shows their brain is being perfused and their cognition improves.
From a vascular point of view, it’s really simple: if you don’t give the cells the oxygen and nutrients they need, they become dysfunctional. They way to provide what they need is through a healthy circulatory system, which produces NO on demand to perfuse the tissues and organs when needed and limit the flow when it is not needed. We don’t have enough blood in our body to equally perfuse all the cells and tissues at any given time—that’s why we regulate blood flow, which is dictated by the production of NO. When you can’t make NO, you lose regulation, and bad things happen.
References
[1] Bryan NS. Nitrite in nitric oxide biology: cause or consequence? A systems-based review. Free Radic Biol Med. 2006 Sep 1;41(5):691-701.
[2] Ma L, et al. Nitrate and Nitrite in Health and Disease. Aging Dis. 2018 Oct 1;9(5):938-45.
[3] Milkowski A, et al. Nutritional epidemiology in the context of nitric oxide biology: a risk-benefit evaluation for dietary nitrite and nitrate. Nitric Oxide. 2010 Feb 15;22(2):110-9.
[4] Hakim TS, et al. Half-life of nitric oxide in aqueous solutions with and without haemoglobin. Physiol Meas. 1996 Nov;17(4):267-77.
[5] Sebranek JG, Bacus JN. Cured meat products without direct addition of nitrate or nitrite: what are the issues? Meat Sci. 2007 Sep;77(1):136-47.
[6] Cross AJ, et al. A prospective study of meat and fat intake in relation to small intestinal cancer. Cancer Res. 2008 Nov 15;68(22):9274-9.
[7] Abete I, et al. Association between total, processed, red and white meat consumption and all-cause, CVD and IHD mortality: a meta-analysis of cohort studies. Br J Nutr. 2014 Sep 14;112(5):762-75.
[8] Rohrmann S, Linseisen J. Processed meat: the real villain? Proc Nutr Soc. 2016 Aug;75(3):233-41.
[9] Loh YH, et al. N-Nitroso compounds and cancer incidence: the European Prospective Investigation into Cancer and Nutrition (EPIC)-Norfolk Study. Am J Clin Nutr. 2011 May;93(5):1053-61.
[10] Oostindjer M, et al. The role of red and processed meat in colorectal cancer development: a perspective. Meat Sci. 2014 Aug;97(4):583-96.
[11] Stellman SD, et al. Smoking and lung cancer risk in American and Japanese men: an international case-control study. Cancer Epidemiol Biomarkers Prev. 2001 Nov;10(11):1193-9.
[12] Samet JM, et al. Cigarette smoking and lung cancer in New Mexico. Am Rev Respir Dis. 1988 May;137(5):1110-3.
[13] Hammond EC, et al. Asbestos exposure, cigarette smoking and death rates. Ann N Y Acad Sci. 1979;330:473-90.
[14] Nuñez De González MT, et al. Survey of residual nitrite and nitrate in conventional and organic/natural/uncured/indirectly cured meats available at retail in the United States. J Agric Food Chem. 2012 Apr 18;60(15):3981-90.
[15] Sindelar JJ. What’s the Deal with Nitrates and Nitrites Used in Meat Products? Meat Science & Muscle Biology Lab, University of Wisconsin [cited 2019 Aug 17]. Available from https://fyi.extension.wisc.edu/meats/files/2012/02/Nitrate-and-nitrite-in-cured-meat_10-18-2012.pdf
[16] Parthasarathy DK, Bryan NS. Sodium nitrite: the “cure” for nitric oxide insufficiency. Meat Sci. 2012 Nov;92(3):274-9.
[17] Hernández-Ramírez RU, et al. Dietary intake of polyphenols, nitrate and nitrite and gastric cancer risk in Mexico City. Int J Cancer. 2009 Sep 15;125(6):1424-30.
[18] Kapil V, et al. Physiological role for nitrate-reducing oral bacteria in blood pressure control. Free Radic Biol Med. 2013 Feb;55:93-100.
[19] Govoni M, et al. The increase in plasma nitrite after a dietary nitrate load is markedly attenuated by an antibacterial mouthwash. Nitric Oxide. 2008 Dec;19(4):333-7.
[20] Bryan NS, et al. Oral Microbiome and Nitric Oxide: the Missing Link in the Management of Blood Pressure. Curr Hypertens Rep. 2017 Apr;19(4):33.
[21] McDonagh ST, et al. The Effects of Chronic Nitrate Supplementation and the Use of Strong and Weak Antibacterial Agents on Plasma Nitrite Concentration and Exercise Blood Pressure. Int J Sports Med. 2015 Dec;36(14):1177-85.
[22] Wang YF, et al. Proton-Pump Inhibitor Use and the Risk of First-Time Ischemic Stroke in the General Population: A Nationwide Population-Based Study. Am J Gastroenterol. 2017 Jul;112(7):1084-93.
[23] McKnight GM, et al. Chemical synthesis of nitric oxide in the stomach from dietary nitrate in humans. Gut. 1997 Feb;40(2):211-4.
[24] Ghebremariam YT, et al. Unexpected effect of proton pump inhibitors: elevation of the cardiovascular risk factor asymmetric dimethylarginine. Circulation. 2013 Aug 20;128(8):845-53.
[25] Andersson KE. Erectile physiological and pathophysiological pathways involved in erectile dysfunction. J Urol. 2003 Aug;170(2 Pt 2):S6-13; discussion S13-4.
[26] Musicki B, et al. Endothelial nitric oxide synthase regulation in female genital tract structures. J Sex Med. 2009 Mar;6 Suppl 3:247-53.
[27] Shifren JL, al. Sexual problems and distress in United States women: prevalence and correlates. Obstet Gynecol. 2008 Nov;112(5):970-8.
[28] Muntner P, et al. Potential US Population Impact of the 2017 ACC/AHA High Blood Pressure Guideline. Circulation. 2018 Jan 9;137(2):109-118.
[29] Thompson IM, et al. Erectile dysfunction and subsequent cardiovascular disease. JAMA. 2005 Dec 21;294(23):2996-3002.
[30] Shamloul R, Ghanem H. Erectile dysfunction. Lancet. 2013 Jan 12;381(9861):153-65.
[31] Bryan NS, Grisham MB. Methods to detect nitric oxide and its metabolites in biological samples. Free Radic Biol Med. 2007 Sep 1;43(5):645-57.
[32] Aranke M, et al. Towards nitric oxide based diagnostics: call to action. Trends Mol Med. 2011 Nov;17(11):614-6.
[33] Arrebola-Moreno AL, et al. Noninvasive assessment of endothelial function in clinical practice. Rev Esp Cardiol (Engl Ed). 2012 Jan;65(1):80-90.
[34] Itimar Medical. EndoPAT Main [Internet]. Caesarea, Israel: Itamar Medical Ltd. [cited 2019 Aug 17]. Available from: https://www.itamar-medical.com/endopat-main/
[35] Bryan NS. The potential use of salivary nitrite as a marker of NO status in humans. Nitric Oxide. 2015 Feb 15;45:4-6.
[36] Torregrossa AC, et al. Nitric oxide and geriatrics: Implications in diagnostics and treatment of the elderly. J Geriatr Cardiol. 2011 Dec;8(4):230-42.
[37] Stephan BCM, et al. Cardiovascular Disease, the Nitric Oxide Pathway and Risk of Cognitive Impairment and Dementia. Curr Cardiol Rep. 2017 Aug 11;19(9):87.
[38] Balez R, Ooi L. Getting to NO Alzheimer’s Disease: Neuroprotection versus Neurotoxicity Mediated by Nitric Oxide. Oxid Med Cell Longev. 2016;2016:3806157.




6 Comments. Leave new
Hi there, What are your thoughts on the nitric oxide spray? I know, not the way to get up your levels naturally but my Dad has it for his angina and if it is too late to get his NO levels up naturally, or I struggle to get him to do so, could this at least help in some way?
Thanks, Susan
Fascinating article. I’m wondering if low NO can be related to Neuro cardio genetic syncope where it is said that the heart and brain don’t communicate… leading to dizziness. Also, would a fullness feeling in the ears (particularly during exercise) be related to inadequate blood flow or low NO levels?
“When you can’t make NO, you lose regulation, and bad things happen.”
Your last statement. I may have been deficient for years, once discovered I showed no color on the stick 1 1/2 yr ago. Now light pink. But suffering. So “bad things” like legs or muscles or thighs? I was overdosed on hormones trying to compensate for fatigue is my guess. So felt weird sensations mostly in my legs 5 years ago. Eventually I would fatigue out in my legs walking across a large parking lot. Now just walking in my condo and lately worse. Can it be reversed? I suspect Formaldehyde poisoning from construction of home I lived in 1974 to 1989. Can you tell me what else I could read? Thank you. Carolyn
What a great article, thank you!
Can you share the names of the NO producing bacteria please?
This is incredibly important news. It shows that just as pesticides are responsible for creating malnutrition and obesity, toothpaste may well be responsible for creating the covid pandemic. I looked up this paper while reseraching the latest drug, nitric oxide, sprayed up the nose, to prevent covid. From what you are saying, we only need this drug because we are already poisoned.
This was an excellent read, thank you! I made it here because I was researching my genetic data results which showed that I may have a dysfunctional enzyme which is a cofactor in the production of nitric oxide. Sure enough, I have all of the endothelial dysfunction symptoms. I’m excited to try and boost my NO and see if there is improvement. This information could also be very helpful for POTS/dysautonomia, which I also have. I will share the information, thank you!